THE
LA RAZA INVASION:
The Washington-imposed economic policy of
economic growth via mass-immigration floods the market with foreign labor, spikes profits and Wall Street values by cutting salaries for manual and skilled labor offered by
blue-collar and white-collar employees. It also drives up real estate prices, widens wealth-gaps, reduces high-tech investment, increases state and local tax burdens, hurts kids’ schools and college education, pushes Americans away from high-tech careers, and sidelines at least 5 million
marginalized Americans and their families, including many who are now
struggling with opioid addictions. NEIL
MUNRO
A NATION DIES OF OPIOID
ADDICTION
AMERICAN BIG PHARMA,
RED CHINA and NARCOMEX PARTNER FOR THE BIG BUCKS
“The drug epidemic is the product of capitalism and the
policies of the capitalist parties, both Democrats and
Republicans. There is, first of all, the role of the pharmaceutical
companies, which have amassed huge profits from the
deceptive marketing of opioid pain killers, which they claimed were
not addictive. Prescriptions for opioids such as Percocet, Oxycontin
and Vicodin skyrocketed from 76 million in 1991 to nearly 259 million in
2012. What are the numbers and profits now?
OPIOID AMERICA: CHINA AND MEXICO
PARTNER TO ADDICT AMERICA
http://mexicanoccupation.blogspot.com/2018/08/the-opioid-war-on-america-chin
PRINCETON REPORT:
American middle-class is addicted,
poor, jobless and suicidal…. Thank the corrupt government for surrendering our
borders to 40 million looting Mexicans and then handing the bills to middle
America?
OPIOID MURDERS BY BIG
PHARMA
“While drug distributors have paid a total of $400 million in fines over the past 10 years, their combined revenue during this same period was over $5 trillion.”
“Opioids
have ravaged families and devastated communities across the country.
Encouraging their open use undermines the rule of law and will do nothing to
quell their continued abuse, let alone the problems underlying mass addiction.”
AMERICA: MEXICO’S WELFARE STATE
… and in exchange we get 40 million Mexican flag
wavers, homelessness, a housing crisis, heroin & opioid crisis and jobs for
legals crisis…. ALL THANKS TO THE DEMOCRAT PARTY
http://mexicanoccupation.blogspot.com/2013/08/how-cheap-is-staggering-cost-of-mexicos.html
“Thirteen years after welfare reform, the share of immigrant-headed households (legal and illegal) with a child (under age 18) using at least one welfare program continues to be very high. This is partly due to the large share of immigrants with low levels of education and their resulting low incomes — not their legal status or an unwillingness to work. The major welfare programs examined in this report include cash assistance, food assistance, Medicaid, and public and subsidized housing.” Steven A. Camarota
Opioid Epidemic Highlights Twisted
Machinery of Foster Care System
February 24, 2019 Updated: February 24, 2019
Millions of Americans recovering from drug addiction amid the opioid crisis face a looming danger of losing their children as social workers are tempted by twisted incentives to separate families even over smaller lapses in parental judgement.
With 20 million Americans needing addiction treatment (pdf) and more than two million hooked on opioids, many families struggle to maintain a wholesome environment for their children. With federal funding on the line, even well-meaning workers of the Child Protective Services (CPS) are then nudged to label parents unfit and funnel hundreds of thousands of children to the shelter and foster care system, where the children often end up faring even worse, at times facing abuse.
Last year’s federal legislation pushed the system somewhat in the right direction, but much work remains, multiple stakeholders made clear to The Epoch Times.
For Michael Ardt, 42, and Janice Ardt, 40, it went down like this:
In December 2014, the couple was taking care of their friends’ three children for two weeks in Kentucky when the police and local Department for Community Based Services (DCBS) workers knocked on the door.
“Someone called in on our friends saying there were drugs in the home,” Janice told The Epoch Times via email.
Oblivious to the seriousness of the situation, they let the police in and even agreed to undergo a drug test. No drugs were found in the house, but the test came back positive for methamphetamine.
The DCBS took their 13-year-old son as well as their friends’ three children.
The three children were at school at the time. Their son wasn’t even staying at the house—he was staying with the Ardts’ adult daughter at the time. And the Ardts weren’t actually drug addicts anymore—as was later confirmed in court, they said. However, in the government’s eyes, they were already bad parents, and despite years of efforts, they never got their son back.
Positive Test
It’s not that CPS is removing children for no reason at all. However, often it’s hard to see a sense of proportion in the actions of the state agencies that operate on a mix of state and federal funding.
In fiscal 2017, there were over 440,000 children in the foster care system. CPS alleged physical abuse in only 12 percent of the cases. Sexual abuse pertained to 4 percent and housing to 10 percent, according to data by the federal Department of Health and Human Services (pdf).

In nearly two thirds of the cases, parents were accused of neglect—a nebulous term with broad definitions that differ from state to state.
In general, neglect means some physical or emotional needs of a child aren’t met. But the CPS workers sometimes resort to inane arguments to prove their case, as demonstrated by the high-profile case of “baby Dylan” in Connecticut.
“Is a 4-year-old eating a piece of cake without sitting at the table, or a small child climbing on a picnic table, or a child eating sweets before enough dinner a safety concern?” The Day’s Deborah Straszheim reported in 2017. “The [CPS] employee said it was.”
Drug use of parents is another major factor in neglect accusations, involved in more than a third of CPS removals.
“If we can get the parent to admit to anything with regards to drugs, we … get the removal,” said former CPS investigator in Texas Carlos Morales, author of the “Legally Kidnapped: The Case Against Child Protective Services,” in a 2013 Youtube video.
“If you admit using marijuana on a weekend when you work with the kids that’s considered emotional and physical neglect and that can lead to the removal of children,” he said.
In the Ardts’ case, the couple was recovering from an opioid addiction sparked when Michael was prescribed pain pills after a neck injury. As is common for opioid abusers, they turned to taking the pills for the high and quickly ended up with physical dependency—something the drug companies pushing the pain pills claimed wouldn’t happen.
The sickening withdrawal symptoms are commonly alleviated with prescribed medication, like methadone, but the Ardts had a different, much more dangerous approach: every now and then, perhaps once in a few months, they would take methamphetamine.
“[It] worked for us although was not the right way to approach it,” Janice acknowledged.
They never did it with children around. “I’m not saying that justifies testing positive, but it doesn’t make us bad or unfit parents,” she said.
It did in the DCBS’s eyes. The agency didn’t respond to a request for comment.
Why Would They Do It?
Research has persistently showed that children coming out of the foster care system have substantially worse life outcomes than children in general. Moreover, an extensive study that came out in 2007 indicated that in marginal cases of neglect and abuse, where both keeping the family together and removing the child was a plausible option, the children that stayed with parents still did better than those removed.
Then, with all the heartache of breaking up a family, why would CPS workers do so unless absolutely necessary?
The situation was perhaps best explained by former Georgia state Senator Nancy Schaefer in her 2007 report “The Corrupt Business of Child Protective Services.”
“The funding continues as long as the child is out of the home,” she said (pdf).
For decades, the system has generally worked as follows:
- The CPS gets a tip that a child may be abused or neglected.
- A CPS worker may visit the family, collect some information, and write an affidavit to a family court—no further evidence necessary—to obtain a removal order. If CPS deems the case serious, it may proceed with removal and obtain the order later.
- The CPS picks up the child from school or daycare, which is required to surrender the child. The CPS may also come to the home accompanied by police and take the child away. The child is sent to a shelter or a foster parent, who gets paid hundreds of dollars a month to care for the child.
- The parents, often on the brink of emotional breakdown, hire a lawyer who tells them they have to do what the CPS tells them to or they may never see their child again.
- The parents protest the removal in the family court and are de facto deemed guilty until proven innocent—they have to prove that the CPS was wrong.
- The CPS prepares a “case plan,” which lists what the parents have to do to get their child back or even get permission to see the child. The plan commonly includes things like therapy sessions, parenting classes, anger management classes, psychological evaluations, and addiction treatment. Some of the services may be government-sponsored, but many the parents need to pay for. In many cases, the CPS would contract with providers of the services and parents would be required to use those providers.
- If a child remains in foster care for more than 15 of the past 22 months, the CPS may start a court case to terminate parental rights and put the child up for adoption, even if the parents’ case against the removal is still in progress.
The federal government pays about half of CPS expenses and the longer the child stays in the system, the more resources are consumed, the more services are provided, the more case workers and lawyers are hired, and the more federal dollars flow in.
Since the 1997 Adoption and the Safe Families Act, pioneered by then-first lady Hillary Clinton, the federal government even offers cash bonuses to the states for every child they adopt out of foster care. The stated idea of the measure was to get children out of foster care sooner because adopted children, research suggests, do better than those in foster care. Yet the bonuses created an incentive to keep as many children as possible in foster care for at least 15 months, so that they could be potentially offered up for adoption.
“In order to receive the ‘adoption incentive bonuses,’ local child protective services need more children,” Schaefer said. “They must have merchandise (children) that sell and you must have plenty of them so the buyer can choose.”
Nearly $680 million was paid out in incentives by the end of fiscal 2017.
Schaefer was found shot dead in 2010 along with her husband. Police said the husband killed her and then himself, but no motive was found.
While the federal funding may be a pressure for CPS supervisors, CPS investigators and case workers are not necessarily aware of how their salary is sourced. They have their own pressures, however.
Morales said he would get a monthly evaluation in which the number of removals would count toward a salary hike at the end of the year.
“The person who removes three kids in a week, well that person’s applauded. The person who prevents three children from being removed in a week, well that person’s called lazy,” he said.
The system is set up in a way that every level of the bureaucracy can simply blame their supervisors, he said.
“You can always blame any kind of inaccuracies or terrible atrocities that occur on someone else,” Morales said.
Regardless of motivation, the incentives appear to have moved the needle over time.
More than a quarter of the children in the foster care system remain in there for over two years. The average time spent in the system is over 20 months.
Adoptions out of the foster care system nearly doubled after the Adoption and Safe Families Act—from 31,000 in 1997 to more than 58,000 in fiscal year 2017.
The number of children exiting the system by reuniting with their parents dropped from 55 percent in 2003 (pdf) to 49 percent in 2017 (pdf). Meanwhile, exits through adoption increased from 18 percent to 24 percent.
In short, the CPS has run on removals, not on the number of parent-child relationships they were able to rehabilitate.
However, there is a sign of hope.
In February 2018, Republicans in the House of Representatives slipped into the 2018 budget bill the provisions of the Family First Prevention Services Act. The bill allows the federal government to use the foster system funding on services that help prevent a child’s removal from their family and help families stay together. Now it’s up to the states to put those programs in place.
By Kate Randall
“Deaths of despair” continue to soar
US deaths from alcohol, drugs and suicide at all-time high
By Kate Randall
8 March 2019
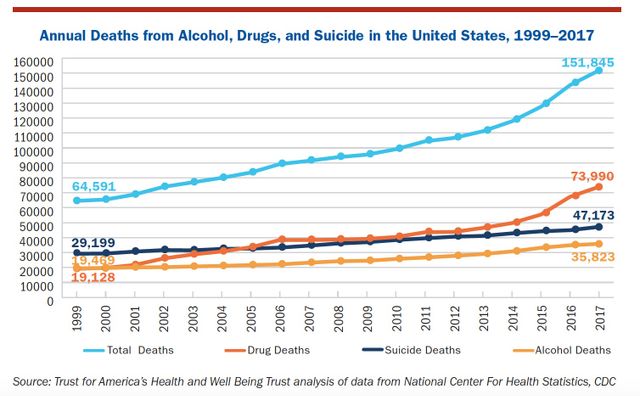
More than 150,000 Americans died from alcohol and drug-induced fatalities and suicide in 2017. This is more than twice as many as in 1999 and the highest number since recordkeeping began in that year. This skyrocketing rate of so-called deaths of despair was confirmed in a new analysis released this week by Trust for America’s Health (TFAH) and Well Being Trust (WBT).
TFAH and WBT analyzed data from the Centers for Disease Control and Prevention (CDC) between 2016 and 2017 and found that the national rate for deaths due to alcohol, drugs and suicide increased 6 percent over that year, from 43.9 deaths per 100,000 to 46.6 deaths per 100,000. While the rate of increase is lower than in the previous two years, it is still higher than the 4 percent average annual increase since 1999.
The new analysis provides insight into the CDC’s findings last years that showed a drop in life expectancy from 78.7 years to 78.6 years, the third consecutive year-on-year decline. In the years since the 2008 financial crisis many workers and their families have confronted an unprecedented crisis of social misery, which is literally cutting life out from under them.
Certain groups of Americans have been hardest hit by the “deaths of despair” examined in the new analysis:
• Ages 35–54: The rate of death from alcohol, drugs and suicide was 72.4 per 100,000. This was a 35 percent increase over 2007 figures.
• Males of all ages: A death rate of 68.2 deaths per 100,000 was found among men.
• Regional disparities: West Virginia, with 81 deaths per 100,000, and New Mexico, with 77, had the highest rates of “deaths of despair” among the 50 US states.
Death by suicide
The suicide rate in 2017 was 4 percent higher than in 2016, rising from 13.9 deaths per 100,000 to 14.5 deaths per 100,000. In 2017, 47,200 Americans died as a result of suicide. Deaths by suicide were particularly high among males (22.9 per 100,000), whites (16.6 per 100,000) and people living in rural areas (19.4 per 100,000)
Over the past decade suicide rates increased by 22 percent. Suffocation and hanging suicides have risen by 42 percent since 2008, while firearm suicides saw a 22 percent increase. These methods are often chosen by suicide victims over less violent means because they are more likely to result in death.
One of the most disturbing trends over the last decade has been the rise is deaths by children ages 1–17. Although suicide deaths in 2017 were still lower than for other age groups, at 2.4 per 100,000, they have risen by 16 percent since 2016. Over the last decade, 12,660 youth under the age of 17 took their own lives, according to the CDC.
Suicide rates over the past decade have also increased proportionally more among blacks (30 percent rise) and Latinos (36 percent) than among other racial and ethnic groups.
Research published by the CDC last year showed that the overall suicide rate increased by 25 percent across the US over the two decades ending in 2016. These figures paint a picture of a social crisis driving increasing numbers of people, both young and old, to take their own lives in the face of personal crises, mental health issues, substance abuse and economic despair.
In 2017, 35,800 Americans died of alcohol-induced causes. The TFAH/WBT report included deaths from alcohol induced causes, including alcohol poisoning, liver and other diseases. It did not include alcohol-related vehicle accidents, violence or accidental fatalities.
Alcohol-induced deaths rose 2 percent in 2017 over 2016, the smallest increase since 2008–2009. The alcohol death rate has increase by 38 percent since 2008. Alcohol-related deaths were highest among males (16.2 per 100,000), whites (12.2 per 100,000), adults ages 55–74 (26.4 per 100,000) and in rural areas (13 per 100,000).
People 55–74, who should be enjoying their retirement, instead are abusing alcohol in record numbers. Those 18–34—who should be gainfully employed, studying or embarking on new careers—have seen a 69 percent rise in alcohol-related deaths over the past decade, as they suffer through unemployment, layoffs and drown in college debt.
Drug deaths
The synthetic opioids fentanyl and carfentanil are 50 to 100 times and 10,000 times more potent than morphine, respectively. Natural/semisynthetic opioids include hydrocodone, oxycodone, morphine and heroin.
Two decades ago, synthetic opioids were responsible for less than 10 percent of all drug deaths in the US. In 2017, they accounted for 38 percent of all drug deaths, with an average of 547 Americans succumbing to opioid overdose deaths every week .
The synthetic opioid crisis has taken its toll on every segment of American society, but has especially hit males (with 12.8 deaths per 100,000 in 2017), blacks (8.6 deaths per 100,000), whites (9.5 deaths per 100,000), adults ages 18–54 (15.2 deaths per 100,000) and those living in metropolitan areas.
A recent study showed that opioid overdose death rates among US teens and children have tripled over the past 17 years. The study, published online in JAMA Network Open, found that young children died from either accidentally ingesting narcotics or from intentional poisoning. Teens more often died from unintentional overdoses, using prescription painkillers found in their homes or drugs bought on the streets.
The Northeast region had the highest opioid mortality rate in 2017 (15.7 deaths per 100,000), followed by the Midwest (12.1 deaths per 100,000). Drug deaths in the Midwest, which includes the Rust Belt ravaged by industrial decline, saw a 122 percent increase in all drug deaths from 2007 to 2017.
The surge in synthetic drug deaths must be laid at the feet of the multibillion-dollar pharmaceutical companies, who have flooded neighborhoods with these potent opioids. Drug companies have pushed prescription narcotics through bribing doctors to prescribe the addictive substances, and by secretly and deliberately increasing their addictive properties.
While politicians of both big business parties have feigned outrage at such practices, they are on the payroll of Big Pharma, receiving millions of dollars from drug company lobbyists. In 2018 alone, the pharmaceutical and health products industry spent a record $280 million on their lobbying efforts.
The war against the health and lives of American workers has been a bipartisan conspiracy conducted over decades as part of a conscious strategy to claw back the gains of the working class begun over a century ago.
For the 150,000 Americans who died from alcohol and drug-induced fatalities and suicides in 2017, millions more have been affected—family, friends, co-workers. But for politicians in Congress and pharmaceutical CEOs this devastating toll is seen as the “cost of doing business.”
The US health care crisis—exemplified by these “deaths of despair” and falling life-expectancy—is a true national emergency, in contrast to the “national emergency” on the Southern US border fabricated by Donald Trump and his fascistic advisers.
The epidemic of alcohol-, drug- and suicide-related deaths is a social crisis that requires a socialist response. Such social misery cannot be battled under conditions where the health and welfare of the vast majority is subjugated to the private wealth of the pharmaceutical and insurance companies and giant healthcare chains. These capitalist enterprises must be expropriated, transformed into public utilities and run on the basis of social need, not profit.
No comments:
Post a Comment