With officials acknowledging that two people who died last week were infected by coronavirus COVID-19, the official number of deaths in the United States has reached nine, with all of the fatalities in the Seattle suburb of Kirkland, Washington. There are now more than 115 known cases of coronavirus in at least a dozen US states. Internationally the number of known cases is approaching 100,000 with at least 3,000 deaths.
The Trump administration, primarily concerned with the impact on the stock market, has sought to downplay the seriousness of the threat to public health. It is apparent, however, that American society is unprepared and ill-equipped to handle the spreading virus.
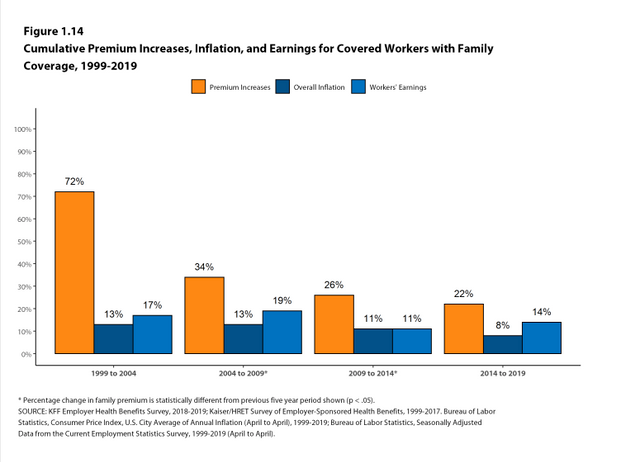
Like every other crisis, whether triggered by hurricanes, tornados or other natural disasters or the global financial crash of 2008, it is the working class which will be most impacted by the coronavirus. The lack of a basic social safety net in the US, high levels of poverty and the proliferation of low-paid and precarious employment have combined with the growth of the uninsured and underinsured population and inability of workers to take time off, even when sick, to create a perfect storm.
 Detroit teachers sickout protests in 2016 to demand improved school conditions
Detroit teachers sickout protests in 2016 to demand improved school conditions
In workplaces, supervisors have given workers little, if any, instructions and it is clear no plans are in place. If schools were closed, like the one-month shutdown in Japan, workers have no idea who would care for their children or how they would afford it. With little or no paid leave, workers have no idea where their income would come from if they were furloughed. Tens of thousands of airline workers could face layoffs because of curtailed travel along with manufacturing workers if components from the global supply chain dry up.
Autoworkers who spoke to the World Socialist Web Site in Detroit expressed particular concern about the danger. The pandemic started in Wuhan, a major manufacturing center, known as China’s “Motor City.”
“Management hasn’t given us any instructions concerning the coronavirus,” Michael, a young Fiat Chrysler worker at the Sterling Heights Assembly plant in suburban Detroit, told the WSWS. “The last company notice we got was about highway construction, but that was just so we don’t show up late for work.
“If the coronavirus hit this plant everyone would get it. We’re supposed to wash our hands but the bathrooms in the plant are filthy and we’re always fighting just to get soap in the dispenser,” he said.
“If this virus got into the plant everyone would get sick,” Anthony, a young Fiat Chrysler worker at the Jefferson plant in Detroit, said, “No one can take a day off when they are sick. It’s insane. A fast food worker gets the virus and comes to work, and we have zero chance of not getting it.
“Hand sanitizers are good, but they can’t solve the issue. It’s like bringing cases of water to Flint when the underlying problem is that the water is full of lead. There are so many uninsured Americans that people won’t even go to the doctors to find out if they have it because it costs too much. There was a joke around social media, which said if you want to find out if you have coronavirus cough on a rich person and see what their doctor tells them.”
After decades of deindustrialization and wage-cutting aided and abetted by the unions, some 220,000 Detroiters, or one in three city residents, and half of the city’s children live below the government’s official poverty line. In Michigan, approximately 535,000 residents were uninsured in 2018, up by 25,000. Far more are underinsured, i.e., they are covered by employer-sponsored insurance plans but cannot afford the premiums, deductibles, co-pays and other out-of-pocket costs.
 Out-of-pocket health care costs have steadily risen even as wages stagnated (Source: Kaiser Family Foundation)
Out-of-pocket health care costs have steadily risen even as wages stagnated (Source: Kaiser Family Foundation)
A 2019 survey conducted by the Los Angeles Times and the Kaiser Family Foundation found that 40 percent of Americans with employer-sponsored health coverage still had difficulty affording the health plan or treatment. Average deductibles for employer-sponsored single coverage tripled from $584 in 2006 to $1,655 in 2019, according to a separate Kaiser study.
How many residents would forgo a trip to the doctor, where the virus could be caught, because they could not afford it?
While government officials are telling people that the best way to prevent the spread of infection is to thoroughly wash their hands, last year Detroit water officials disconnected 23,500 residents because they could not afford to pay their bills. As of January 15, 9,500 of those were still without water, according to city records.
Last week, Michigan’s Democratic governor, Gretchen Whitmer, rejected an appeal by the American Civil Liberties Union and Detroit civic groups that she use emergency powers to halt the water shutoffs because of the threat to public health.
On Monday, Nikolai Vitti, the superintendent of the Detroit Public Schools Community District, sent a perfunctory email to teachers and support staff trying to allay concerns and fears of the potential impact on the 50,000-student school district. “Public health officials continue to advise that the risk to the public remains low,” Vitti writes, before instructing workers and their families to “practice good hygiene habits,” including “wash your hands for at least 20 seconds” and “stay home when you are sick.”
One Detroit teacher commented, “The problem with teachers and students being told to wash their hands is that many schools do not have soap. This is widely known and was one of the reasons for the teacher sickouts in 2016. The lack of supplies has still not been resolved.
“We don’t know which of our families do or do not have water. So, we have to anticipate that many of the students come to school without washing because their water was shut off. In school, we insist they wash their hands, but the water is poisoned with lead. So whatever advantages they get by getting rid of germs and virus, now we have to worry about their skin absorbing the lead through their skin, especially if they have abrasions or cuts.
“Parents are frequently working two or three jobs and they don’t have sick leave or other paid time off and often send their children to school sick. Not all schools have school nurses. Even for those that do, if the nurses screen the child for fever or other illness, it is not guaranteed that the parent will be able to get off of work and pick them up. If there is a school with 500–1,000 students and you have one student who is infected with coronavirus, it has the potential to be spread to all the students and their families, and to grow exponentially. This is especially true in an impoverished city like Detroit where going to an urgent care center or hospital emergency room is not affordable or easily accessible.”
In a February 29 article entitled, “If coronavirus sweeps America, blame our brutal work and healthcare culture,” Los Angeles Times business columnist Michael Hiltzik noted when the H1N1 flu virus hit the US in 2009, an estimated 26 million residents were infected during its peak months. Of these, an estimated 8 million continued to go to work while they were sick. “By the following February, public health authorities reckoned that those carriers infected some 7 million co-workers,” the Times wrote, adding, “The problem was especially acute in the private sector, where paid sick leave was relatively rare.”
The phenomenon of working while sick is so common that US businesses have a term for it, “presenteeism.” The primary concern expressed by corporate management is how illnesses or other physical ailments undermine workplace productivity.
A study by Pennsylvania State University cited by the Times concluded, “Presenteeism—attending work while ill—among private sector employees without paid sick days may have extended the duration of the [2009 flu] outbreak.”
A quarter of American workers have no right to sick leave, according to the Bureau of Labor Statistics. Only 58 percent of service workers, less than half of those in the lowest 25 percent of the income range, and only three in 10 of those in the lowest 10 percent of wage earners have sick leave, the Times notes.
As opposed to other countries, where many workers receive paid sick leave, in the US time off is often unpaid. In Britain, “workers are entitled to sick pay of at least $120 a week for up to seven months, at their employer’s expense. In France, the government and employers together cover 90% of a worker’s pay for up to 30 days of sick leave, 67% after that,” the Times notes.
“In China, the epicenter of the developing outbreak, workers are guaranteed 60% to 100% of their salary for up to six months, depending on their seniority, and 40% to 60% for up to six years after that. Those liberal standards may have eased the pain for workers when authorities imposed stringent quarantines in Wuhan province, where the virus is thought to have originated.”
The coronavirus emergency has revealed the entirely irrational character of the capitalist system, which subordinates every aspect of life to the relentless pursuit of profit by giant corporations and blocks society from marshaling its scientific, technological and human resources around the world to combat this threat to public health. This underscores the need for the socialist reorganization of society, based on human need, not profit.
“Big Pharma will protect their profits by any means necessary,” a veteran Fiat Chrysler worker in Detroit declared. “All the countries should come together to tackle this. We need global healthcare.”
Coronavirus kills at more than 20 times the rate of seasonal flu
The World Health Organization (WHO) announced on Tuesday that the mortality rate for reported cases of COVID-19 has risen to 3.4 percent, based on the ratio of the current number of deaths caused by the virus to the confirmed infections. At the time of the announcement, those figures stood at 3,254 and 95,184, respectively.
The coronavirus fatality rate is more than 20 times the death rate of the seasonal flu, according to data from the US Centers for Disease Control and Prevention (CDC)—a stark measure of the dangers the novel coronavirus poses to the world’s population.
This number is an increase over early estimates of the mortality rate by the WHO at just above 2 percent. It reflects the spread of the coronavirus to 83 countries and territories outside of China. The fatality ratio has stayed relatively constant since February 25, even as new cases and new deaths have been confirmed. It is unclear whether the current mortality rate will hold or change in the coming days.
One of the many causes of the spread of COVID-19 is the fact that workers are unable to take sick days, even when exhibiting symptoms of the infection. Chipotle workers in New York City yesterday held a protest against the fast food chain demanding that the company stop forcing workers to work while sick, especially in light of the spread of the coronavirus in the state. They exposed retaliation by the company against workers who stayed home to recover and prevent the spread of the disease in spite of orders by management.
Questions are also being raised as to whether a vaccine will reduce the impact of the disease, especially if it is not distributed freely. Asked at a congressional hearing last week to guarantee that once a vaccine against the virus is developed it will be available to all, US Health and Human Services Secretary Alex Azar, a former pharmaceutical executive, refused. “We would want to ensure that we worked to make it affordable,” he said, “but we can’t control that price because we need the private sector to invest. Price controls won’t get us there.”
As the spread of the coronavirus continues, the WHO is very concerned that the medical supplies necessary to combat the disease could run out. A statement issued by the organization on March 3 warned that “supplies are rapidly depleting.” It said the medical industry had to increase manufacturing by 40 percent if the demands placed upon the world’s health care infrastructure by the pandemic were to be met.
In raw numbers, the world needs 89 million medical masks, 76 million examination gloves, 30 million gowns, 1.6 million goggles and 2.9 million liters of hand sanitizer each month until the pandemic is contained. The WHO has also called for “the rational and appropriate use of personal protective equipment in healthcare settings, and the effective management of supply chains,” after prices for gowns doubled, respirators tripled and surgical masks increased six-fold.
This shortage is especially dangerous in regions with a higher fatality ratio or where coronavirus cases have been surging. While the number of new cases in China dropped to 119 yesterday, South Korea, Italy and Iran reported 435, 587 and 586 new cases, respectively. Those countries also reported 3, 28 and 15 new deaths, raising concerns that COVID-19, given its two week incubation period, has already infected large swaths of those countries.
There are also worries that the virus is much more widespread than currently reported in the United States. To date, 11 out of the 154 known cases have resulted in the patient’s death. Assuming that the average mortality rate of 3.4 percent holds true, the 11 confirmed deaths predict that there are actually 324 cases of the coronavirus in the country, and that 170 of them have gone unreported.
While there are many reasons that an infection of COVID-19 might be missed, the most prominent is the enormous cost for Americans to visit a doctor. Costs for those who have been tested for the coronavirus have reportedly been as high as $3,200.
Moreover, the response by federal, state and local governments to the crisis has been improvised and disorganized at best. The CDC has been unable to provide testing kits on a mass scale for hospitals around the country. Thus far, only 472 tests for COVID-19 have been carried out in the US, as compared to 23,345 in Italy, 109,591 in South Korea and tens of millions in China. The CDC insists that hospitals and laboratories in the US use its testing procedure and equipment, rather than those of the World Health Organization. This has essentially crippled the ability of medical professionals in the US to detect the coronavirus and protect their patients and themselves.
Typical of commentaries on US social media, Twitter user Matt Stoller wrote: “Just spoke with ER doc who say[s] he’s seeing cases he’s 99 percent sure are #coronavirus. Negative for flu, recent travel, work in airports. Not allowed to test. Patients return to work because they can’t take time off w/out a firm diagnosis. Other ER docs seeing the same thing.”
In addition to spreading, there is now evidence that it has developed into different types. A study published Tuesday in the National Science Review found genetic markers indicating that a subset of the virus in Wuhan evolved from a less aggressive S-cov to a more transmittable and deadly L-cov, but that the spread of L-cov was largely curbed by the quarantine of Hubei province.
This is little comfort. Mutations that happen once can happen again. Given the spread of the coronavirus around the world, a version that is more aggressive and lethal has the potential to kill hundreds of thousands and infect tens of millions.
The world’s resources must be mobilized at once against this pandemic to contain the disease, treat the sick and save lives.
takes hold in New York
Developments over the past few days have underscored that New York City, the largest in the United States, may well be on the verge of a medical and social catastrophe. There are now 11 confirmed cases of novel coronavirus infection in New York state, and about 1,000 people are quarantined or self-quarantined in Westchester County, just north of New York City.
Most of the cases are tied to a New Rochelle-based attorney who works in Manhattan with no apparent links to people who traveled to coronavirus hot spots, indicating community spread.
The first confirmed case of COVID-19, the official name of the disease caused by the novel coronavirus, in New York was of a health worker who returned from Iran to Manhattan and shortly after began experiencing symptoms of the disease and was diagnosed on Sunday. She is not currently believed to have transmitted the virus to anyone else.
Earlier this week, the New Rochelle attorney was diagnosed with COVID-19, and on March 4 New York Governor Andrew Cuomo announced that several people tied to the man, including his entire family, the neighbor who drove him to the hospital and his neighbor’s entire family, had been diagnosed as well. About 1,000 people are now quarantined or self-quarantined due to their connections with these cases, including members of the man’s synagogue, where he attended a funeral and a bat mitzvah recently.
Yeshiva University, where the man’s son is a student, and the Bronx high school where the man’s daughter is a student are temporarily closed, and those who interacted with the since-diagnosed children have been ordered to self-quarantine.
Two members of the man’s family are asymptomatic and were only tested for COVID-19 due to their known close connection with the attorney. Given the number of people who exhibit few or no symptoms and the lack of widespread testing, it is highly likely that the disease is much more widespread than presently known, in New York and globally.
The attorney’s coworkers are currently being tested, and it is known that he commuted via Metro-North Railroad, which may have exposed other passengers to the virus. What is known about COVID-19 indicates that it is highly contagious and can spread via respiratory droplets and physical proximity. It also has an incubation of up to 14 days. China’s National Health Commission now recognizes both feces and urine as possible modes of transfer as well, raising new difficulties.
There are other possible cases of the virus in New York, including a New York City public school teacher in self-quarantine after showing symptoms and a Brooklyn man who returned from Tokyo with symptoms yet was not tested while in the hospital because the Centers for Disease Control and Prevention (CDC) said he was not sick enough.
A number of universities in the New York area have canceled nonacademic events and travel, and Governor Cuomo announced that students in New York’s public university systems studying abroad in five countries hit the hardest by the epidemic would be flown back to the US on chartered planes and quarantined for 14 days.
One especially disturbing development in the coronavirus epidemic in New York has been the media’s tendency to fan anti-Chinese xenophobia. The New York Times and the New York Post, in reporting on New York’s first coronavirus case, used photos of Flushing, a well-known neighborhood in Queens with a large Asian-American, especially Chinese-American, population. Both of the photos showed residents who appear to be Asian wearing masks.
Given the facts of the case—a virus contracted in Iran by a patient who lives in Manhattan—along with the fact that presumably those involved in selecting the photos know about New York City, it is hard to believe that these were both honest mistakes. The New York Post is a right-wing, Rupert Murdoch-owned tabloid, while the Times, the liberal “paper of record,” in an October 2019 editorial, denounced the “dangerous and growing threat” posed by the “aggressive … Communist [Chinese] state.”
There are a number of factors that make the US a “perfect storm” in terms of the coronavirus despite its status as the world’s wealthiest country. These include the high cost of healthcare and lack of paid time off. The New York metropolitan area has more undocumented immigrant workers, who have even fewer rights to sick leave than other workers, than any other city in the country.
As of this writing, there are 158 confirmed cases in the US and 11 deaths, all in Washington state with the exception of a death Wednesday in California. The interplay of the “perfect storm” factors helps explain how 11 people have died from COVID-19 while countries with more cases have between zero and six deaths.
New York City combines these factors with a public transit system that is used by over 5 million people daily, by far the largest public transit system in the country. Especially during rush hour, passengers are in close proximity. It is not clear what role this could play in disease transmission, with one study finding that the subway would account for 4 percent of transmission in a flu epidemic.
The Metropolitan Transportation Authority, which runs the subways, buses and commuter rail in and around New York City, has announced Monday that it is disinfecting every subway car and bus every 72 hours in response to the epidemic, and that stations are being cleaned on a daily basis using outside contractors—an expansion of a loophole allowed by the Transport Workers Union in the latest contract.
A number of medical professionals have sounded the alarm on the criminally negligent response of the Trump administration in particular to the epidemic. Matthew McCarthy, a professor at Weill Cornell Medicine and author of Superbugs: The Race to Stop an Epidemic, tweeted Sunday: “Coronavirus has been circulating in the United States for weeks. We didn’t detect it because we weren’t testing it properly. There may have been cryptic transmission in Washington State since January. If I sound alarmed, it’s because I am.”
Howard Forman, a professor at Yale University who teaches radiology and healthcare management, told Business Insider: “It is well within the realm of possibility that there are 100,000 people infected with this right now in the United States. Healthcare providers may be being exposed, other patients may be being exposed, and until you can give confidence to people about those answers, we are in a crisis here.”
When the first case was diagnosed in New York this weekend, the CDC had run fewer than 1,000 tests, despite having several weeks of notice since the novel coronavirus began spreading rapidly in Hubei Province, China, where it is thought to have originated. COVID-19 has spread internationally, with over 80,000 cases in mainland China, over 5,000 in South Korea, about 3,000 each in Italy and Iran, and over a hundred each in Japan, France, Germany, Spain, Singapore, Hong Kong and the US.
In an initial indication of the explosive class implications of the epidemic, workers at the Chipotle restaurant chain protested Wednesday in New York City demanding paid sick days, a crucial demand in any initiative to combat the epidemic. That workers must demand basic rights such as sick time off—all the more necessary during a public health emergency—in the same city as Wall Street firms receiving yet another interest rate cut to inflate the stock market illustrates the inability of capitalism to solve any major issue in a socially progressive way.
Almost half of cancer patients in the
US deplete entire life assets by second year of treatment
A
team of surgeons operate on a patient [Source: Flickr.com]
Healthcare
access has declined in past two decades, despite Obamacare: Study
Almost half of cancer patients in the
US deplete entire life assets by second year of treatment
After a colon cancer
diagnosis, Deb Genetin, a 57-year-old resident of Springfield, Ohio, just
outside Dayton, was denied a life-saving surgery at Mercy Health hospital
because, in the words of the hospital, her “financing wasn’t in place.” Genetin
has not had health insurance in 10 years and makes only $20,000 a year as an
administrative assistant in a law firm.
Last month, Genetin
told the Times-Reporter, “They never told me how much money they
needed, how much money I had to come up with. It was just a ‘No.’” Genetin had
previously applied for financial aid through Mercy Health but was rejected.
Genetin then sought cheaper care at Ohio Valley Surgical Hospital, where she
received the necessary surgery.
While Genetin is
currently cancer-free and now has health insurance, she is struggling to both
meet her payments and pay off medical debt. “I had to drop my hours and my
income to get [health insurance] and now I struggle to pay the house payment,”
she told reporters.
Genetin is one of
thousands of cancer patients in the United States who struggle to afford adequate
treatment. In the last decade, researchers and physicians have begun to further
explore the patient-level financial and health consequences of high-cost cancer
treatment.
A 2018 study from the American Journal of
Medicine (AJM), titled “ Death or Debt? National Estimates
of Financial Toxicity in Persons with Newly-Diagnosed Cancer, ” evaluate d the
extent of financial damage caused by a cancer diagnoses in the United States.
The study ’ s large sample size of 9.5 million is a significant extension of
previous studies that gathered data on a smaller or state level. The data was
pulled from the Health and Retirement Study sponsored by the National Institute
on Aging and Social Security Administration. Data was collected from 1998 to
2014 on people over 50 years old.
Inclusion criteria for
the AJM study involved new cancer diagnoses of any type
excluding minor skin cancer. Based on the year of diagnosis, a baseline financial
value was gathered from two years before the diagnosis to act as a control. The
trajectory of the patient’s finances was examined at two years and four years
following the initial diagnosis. Changes in the patient’s net worth were
calculated based on total wealth, a figure including assets and properties and
subtracting debts such as mortgages and consumer debt.
The study found that
42.4 percent of the 9,527,522 new diagnoses of cancer between 2000 and 2012 had
lost their entire life’s assets by year two. A further thirty-eight percent had
depleted their life assets by year four. The average net worth by year two was
$92,098, depleted from the average initial net worth of $644,031.
Large decreases of net
worth were seen among those with both worsening and improving cancer status.
The largest overall decreases were seen in patients over 75 years old with an
average loss of $115,000. Comorbidities such as hypertension, current smoker,
and lung disease increased the odds of total net worth depletion. Those with
Medicaid as compared to private insurance were independently associated with
financial losses at year two and four.
This is not a new
phenomenon. In 2013, cancer physicians and researchers wrote a two-part
manuscript, “Financial Toxicity: A New Name for a Growing Problem” in which
they coined a new term, “Financial Toxicity,” to describe the patient-level
financial impact of cancer care. The term encompasses both the objective
financial burden on the individual and society as well as the subjective
experience of financial strain during a period of illness and healing. The
inclusion of the word “toxicity” in the term is carefully chosen, as
researchers have found that the financial stress of cancer treatment is a risk
factor for mortality.
In a study titled
“Financial Insolvency as a Risk Factor for Early Mortality Among Patients With
Cancer” published in the Journal of Clinical Oncology in
2016, authors Scott D. Ramsey, Aasthaa Bansal and Polly Newcomb linked cancer
registry records with federal bankruptcy records. A previous study by the same
researchers showed that individuals with cancer are two and a half times more
likely to file for bankruptcy compared to those without cancer. With this
knowledge, the results of the 2016 study are all the more shocking.
While results varied
based on the type of cancer, those who filed for bankruptcy after a diagnosis
of breast, lung, colorectal or prostate cancer had significantly higher
mortality rates. Patients suffering from prostate cancer who filed for bankruptcy
were twice as likely to die. The risk of mortality was 2.5 times as high among
patients with colorectal cancer who filed for bankruptcy compared to those who
did not. While bankruptcy is at the extreme end of financial desperation, other
studies have also found an association between high out-of-pocket costs and
poor clinical outcomes.
There is no one reason
for the correlation between financial toxicity and poor clinical outcomes.
Financial insecurity may lead patients to seek out underfunded hospitals where
risks of infection or medical errors may be higher. Patients may skip doses of
medications or cut pills in half to stretch their prescriptions, in some cases
resulting in subtherapeutic, and thereby insufficient, blood levels of
medications.
Patients forced to
handle large out-of-pocket costs are also more likely to forgo or delay
necessary treatments. Cancer patients often work longer hours or cancel
vacations to cover medical expenses sacrificing periods of rest and putting
undue stress on their bodies during a period of healing. Many lose their jobs
after long hospitalizations, or cannot work due to lowered immune systems or
fatigue, further dragging them into debt and financial distress. For many,
extra expenses for healthy food or even safe, comfortable housing is cut in
order to pay for treatment.
In the US, cancer is
one of the most expensive diseases to treat, second only to heart disease.
According to the
National Cancer Institute (NCI), many chemotherapy agents cost more than
$10,000 a month. Many treatment regimens require multiple chemotherapy drugs
working in tandem, increasing the cost two- or threefold. And the cost is
growing as new pharmacological breakthroughs and treatments carry impossible
price tags.
Immunotherapy, for
example, is a groundbreaking new treatment that activates the body’s immune
system to fight cancer cells. It has been approved in the US and elsewhere as a
first-line treatment for many types of cancer. While typical chemotherapy kills
all cells, immunotherapy is more precise, sparing healthy cells resulting in
fewer side effects and a higher quality of life during treatment. Immunotherapy
also capitalizes on the immune system’s ability to continuously adapt in order
to kill even the most rapidly changing cancer cells. Relapse rates are reduced
with immunotherapy because the immune system has “memory,” and it can remember
cancerous cells and fight them if the cancer returns.
While the development
of immunotherapy is a result of decades of scientific research across the
world—most of which took place in publicly funded institutions—the final,
packaged, life-saving product, is only available to a select few. Without
insurance, immunotherapy costs roughly $100,000 per person when taken for a
year. Like chemotherapy, immunotherapy is often used in combination, which
doubles or triples the cost. One immunotherapy agent, named Kymriah, used as a
one-time dose to treat refractory non-Hodgkin lymphoma and B-cell acute
lymphoblastic leukemia, costs $475,000.
Recent lawsuits against major pharmaceutical
companies have shown that the cost of high-priced drugs are not simply a
product of research and development—as companies claim—nor are the profits they
generate used to fund future innovation. Instead, profits are funneled into
stock buybacks, boosting the company’s stock profiles and increasing the wealth
of the executives.
Even with private
insurance, many patients are denied coverage for immunotherapy or forced to
cover up to 25 percent of the cost. Furthermore, drug costs are just one aspect
of cancer treatment. Hospitalization, teams of specialists, new advancements in
imaging, surgery and radiotherapy collectively contribute to a systemic rise in
cancer treatment cost that shoots past the rate of inflation. At the same time,
average deductible costs for job-based health insurance have increased from $376 in 2006 to $1,300 in
2019. In a country where 70 percent of people live paycheck-to-paycheck, a
single overnight stay in the hospital could deplete a family’s savings.
Young adults, while
less likely to be diagnosed with cancer, face an even higher chance of
financial ruin after diagnoses. With insufficient savings accounts, student
debt, lower-income jobs and lack of eligibility for Medicare, young adult
cancer survivors begin their lives buried in debt, many relying on
crowdsourcing websites like GoFundMe or private charities to stay afloat.
The upsurge in research
on the financial impact of cancer treatment has spurred many health care
workers to advocate for screening patients for financial toxicity as well as
initiating open conversations about the financial stress of treatment. However,
aside from connecting patients with resources like private charities that cover
a limited portion of treatment costs, conversations and awareness about
financial toxicity are not a solution, as the problem finds its source in the
capitalist system and the historic levels of social inequality that it has
produced. Among rich and middle-income countries, the US has some of largest
income-related disparities in health care. In the face of a cancer diagnosis,
this translates directly to financial ruin and higher mortality among poor and
working-class Americans.
Healthcare
access has declined in past two decades, despite Obamacare: Study
Financial access to healthcare services has
declined over the past two decades, despite the implementation of Obamacare and
other government insurance programs, according to a new study.
The analysis, published
in JAMA
Internal Medicine, traces the drop in access to the rise in premiums,
deductibles, co-pays, and other costs, which have weighed against higher
insurance coverage. It concludes that "over the past 20 years, the proportion
of adults aged 18 to 64 years unable to see a physician owing to cost
increased, mostly because of an increase among persons with insurance."
The authors, three
doctors, interpret the results as evidence in favor of government-financed
healthcare.
“With private
insurance, we’ve seen significant worsening in the amount that patients are
expected to pay, like premiums, deductibles, out-of-pocket costs, co-insurance,
and co-pays,” said Dr. Laura Hawks, a researcher at Harvard Medical School and
co-author of the report.
The study finds that
the share of insured adults who had trouble affording the cost of seeing a
physician increased from 7.1% to 11.5% between 1998 and 2017. Meanwhile,
insured people with chronic health conditions struggled frequently to pay for
visits to specialists. About 1 in 5 patients with a chronic medical condition,
such as diabetes or heart disease, said they could not see a doctor because of
high costs. In 2017, for instance, the proportion of insured people who have
chronic conditions, including heart disease, yet were unable to afford a visit
to the doctor was 6.9 percentage points higher than in 1998.
The decline in access
has occurred even though health insurance coverage has risen, from 83.1% in
1998 to 85.2% in 2017.
Hawks said
government-run health plans, such as Medicaid, give people higher-quality
coverage because they lack the same cost-sharing measures as private plans,
including premiums and deductibles, that restrict access to health services.
“Our interpretation Is
that the increased cost-sharing that’s required for private insurance companies
to exist is the reason for these rising costs,” Hawks said. “So, if we were to
reform the healthcare system, we’d want it to be universal as well as
comprehensive, and the only way we could accomplish this is through a
single-payer insurance system.”
Presidential candidates
Bernie Sanders and Elizabeth Warren have each proposed Medicare for All
healthcare plans, which would eliminate all premiums, deductibles, and co-pays
by enrolling everyone living in the United States into a government plan.
Democrats and President
Barack Obama enacted Obamacare to provide access to private health insurance
for people who did not have employer-provided or government insurance plans.
The law did improve access, according to the study. However, a single
middle-class earner making about $48,000 or more annually makes too much money
to qualify for tax subsidies for premiums, making a private plan through the
Obamacare marketplace too expensive for individuals and families.
One of the study's
authors, Dr. David Himmelstein, a public health policy professor at the City
University of New York and a supporter of “Medicare for all," said
Obamacare accomplished a lot but came up short.
“The study is an
endorsement of the fact that we need more reform of the healthcare system, but
it doesn’t suggest a specific reform,” Himmelstein said. “What it says about
[Obamacare] is that it brought more people into the system, but it didn’t fix
the system.”
No comments:
Post a Comment