When Biden took office, one of his first acts was the elimination of our border security. Like a power-hungry dictator, Biden simply decided to ignore our immigration laws. His catastrophic border policy resulted in untold millions of unidentified foreign citizens from around the world pouring into our country. Its impact is now being felt in cities across the country. The worst is yet to come. PETER LEMISKA - AND WE'RE ALREADY THERE!!!
Friday, November 29, 2019
WHY HEALTHCARE SHOULD BE NATIONALIZED
Earlier this year, for the first time, federal prosecutors in
When a stock price rises or has a better P/E ratio, this is generally considered a measure of success. Is this true for health insurance stocks? Stockholders certainly are happy, but what about the purchasers of the carriers’ policies? Are patients smiling when the stock price goes up?
The primary function of any healthcare system is not to save money or to insure people. It is to facilitate timely access to needed care. Having an insurance policy, whether private or government-supplied, is considered the key to a doctor’s office. One might surmise that when an insurance seller does well, so does the insurance buyer.
Is there a relationship between the financial condition of companies that sell health insurance and the people who buy their policies?
Financial Data
The ten-year period of 2007-2017 was chosen as it spans a time before the Affordable Care Act was passed in 2010 and three years after the ACA was implemented. Some market changes could be at least in part attributable to the ACA.
The seven companies listed in Table I represent major sellers of health insurance. Together, they cover more than 128 million Americans (Table I), including more than 4 million with Medicare supplemental policies.
Over the ten years, stock prices rose 157 percent to 635 percent (Table I). During the same period, the S&P 50 increased 82 percent. The one-year forward price/earnings (P/E) in 2007 ranged from 8.27x to 16.44x. By 2017, the P/E ratio has increased in every case, from 17.45x to 23.3x. The one-year relative P/E ratio also increased in five out of seven stocks and decreased slightly in two.
Table I: Sellers of Health Insurance
Company
Stock Price (12/31/year)
Americans covered by company policies*
2007
2017
Change
Anthem
$ 87.73
$ 225.01
↑ 157%
40.8 million
Cigna
$ 53.73
$ 203.09
↑ 278%
11 million
Humana
$ 75.31
$ 248.07
↑ 229%
13 million
UnitedHealthcare
$ 58.20
$ 220.46
↑ 279%
41.6 million
Centene
$ 6.86
$ 50.44
↑ 635%
14 million
Molina
$ 25.80
$ 76.68
↑ 197%
3.5 million
Wellcare Health
$ 42.41
$ 201.11
↑ 374%
4.4 million
S&P 50
$ 1,468.36
$ 2,673.61
↑ 82%
N/A
Yr=year. S&P 50=Standard and Poor’s top 50 companies. (*) published enrollment numbers are from different years, 2015 to 2019.
Access to Care
Two useful metrics of access to healthcare are wait time to see a primary physician and the percentage of physicians willing to accept Medicaid patients. In 2018, 74.8 million Americans were enrolled in Medicaid. People with no identified primary doctor, whether Medicaid or uninsured, tend to forego routine or preventative care and use emergency rooms for care.
In 2007, 74 percent of U.S. physicians accepted new Medicaid patients into their practices. That percentage decreased to 55 percent ten years later. From 2007 to 2017, due largely to Medicaid expansion under the Affordable Care Act, the number of uninsured Americans declined from 47.5 million to 39.9 million.
The maximum wait time to see a primary care physician was chosen rather than the average wait time because medicine is practiced on individuals, not on populations. The patient who waits the longest is most likely to suffer harm from the delay. The maximum wait time in 2007 was 99.6 days. It has increased to 175.7 days.
The change in stock prices and decline in access to care are not merely coincidental. They are statistically related. Pearson’s chi square test (c2=24.5582) indicates a strong correlation, p<0.0001.
Solution
A host of factors influence the price of a stock including general economic conditions, competition, leadership and capitalization of companies, and the regulatory environment. However, all factors culminate in the public perception of future earnings, which affects the price people are willing to pay for a stock.
Evidence suggests a link between a rise in prices of insurance stocks and a decline in patients’ access to care. Health insurance sellers increase profits by (a) not paying for patient care, and/or (b) delaying payments, so the retained earnings can be invested. This “three D” strategy -- delay, defer, or deny care -- generates profits and drives the stock price upward while closing the door to the doctor’s office.
Reduction in availability of care is an adverse impact -- a symptom of healthcare dysfunction. To reverse it, one must identify and treat the root cause, which is the system, not the individuals.
Third-party payment structure is the root cause -- it misaligns the incentives by rewarding the outcome consumers don’t want, less care, instead of incentivizing the desired outcome, access to medical care.
To realign the incentives requires reconnecting buyer (patient) with seller (provider) so the buyer pays the seller directly rather than the third party, government or insurance. When buyers spend their own money instead of OPM (other people’s money), they automatically align the incentives to get what they want: care. When the third party pays, it gets what it wants: profit for insurance carriers and power for the federal government.
Reconnection of buyer and seller is a market-based approach and the antithesis of government-controlled single-payer or Medicare-for-All. For those who would claim that Americans cannot afford to pay for their care, the facts suggest otherwise. In 2018, the average American family spent $28,166 on healthcare costs, representing more than 45 percent of median gross income.
Market-based financing of healthcare would be less expensive and could provide timelier care than the system we currently have or changes in healthcare being planned by Washington.
Social counterrevolution and the decline in US life expectancy
A study published this week in the Journal of the American Medical Association (JAMA) details the fall in life expectancy in the United States from 2015 to 2017, a streak unprecedented in modern times.
Virginia Commonwealth University professor Dr. Steven H. Woolf and Eastern Virginia Medical School student Heidi Schoomaker analyzed life expectancy data for the years 1959-2016 and cause-specific mortality rates for 1999-2017. The data shows that the decline in life expectancy is not a statistical anomaly, but the outcome of a decades-long assault on the working class.
The report exposes a country in the grips of a profound social crisis. The record stock prices touted by Trump are, in fact, a measure of the increased economic exploitation that has produced the fall in life expectancy among workers.
Protesters assemble a makeshift memorial to those lost to drug overdoses last year during a demonstration in support of a proposed supervised injection site, outside the federal courthouse in Philadelphia, in September [Credit: AP Photo/Matt Rourke]
The shuttering of thousands of factories and mines, countless store closures and downsizings, along with the slashing of wages, pensions and health care benefits to meet the demands of Wall Street investors have literally killed hundreds of thousands of workers across the United States.
Life expectancy increased annually from 1959 until it stopped rising in 2010, plateauing at zero growth before beginning its descent after 2014, when it peaked at 78.9 years. By 2017, life expectancy had fallen to 78.6 years.
Not coincidentally, 2010 was also the year that Obamacare was signed into law an attack on health care sold as a progressive reform. The decline in life expectancy since then exposes Obamacare’s regressive character, only one of the reactionary legacies of the Obama administration.
Obamacare was part of a deliberate drive by the ruling class to lower the life expectancy of working people. As far as the strategists of American capitalism are concerned, the longer the lifespan of elderly and retired workers, who no longer produce profits for the corporations but require government-subsidized medical care to deal with health issues, the greater the sums that are diverted from the coffers of the rich and the military machine.
A 2013 paper by Anthony H. Cordesman of the Washington think tank Center for Strategic and International Studies (CSIS) frankly presented the increasing longevity of ordinary Americans as an immense crisis for US imperialism. “The US does not face any foreign threat as serious as its failure to come to grips with… the rise in the cost of federal entitlement spending,” Cordesman wrote, saying the debt crisis was driven “almost exclusively by the rise in federal spending on major health care programs, Social Security, and the cost of net interest on the debt.”
Meanwhile, conditions for the rich have never been better. This is reflected in the growing life expectancy gap between the rich and the poor. The richest one percent of men live 14 years longer than the poorest one percent, and the richest one percent of women 10 years longer than the poorest.
Despite expending far more per capita on health care than other major capitalist countries, the United States has fallen far behind when it comes to life expectancy and mortality. The US began to lose pace with other developed countries beginning in the 1980s, and by 1998 had fallen below the average for countries in the Organization for Economic Cooperation and Development.
The first nodal point, in the early 1980s, corresponds to the initiation of the social counterrevolution by the administration of Ronald Reagan, which involved union busting, strikebreaking, wage-cutting and plant closings on a nationwide scale, combined with cuts in education, health care and other social programs. This was launched with the breaking of the PATCO air traffic controllers’ strike in 1981, carried out with the complicity of the AFL-CIO. Reagan’s social policies were rapidly adopted by the Democrats and continued by the Clinton and Obama administrations.
The second major inflection point was the Wall Street crash of 2008, which was followed by trillions in bailouts for the banks on the one hand and brutal austerity against the working class on the other. The ensuing decade has seen the explosion of the opioid crisis, which has ravaged communities across the United States.
According to the JAMA report, the decrease in life expectancy is the outcome of nearly three decades of increasing mortality among midlife working-age adults, those 25-64. This is mainly the result of a dramatic rise in drug overdoses, alcohol abuse, suicide and a series of organ system diseases.
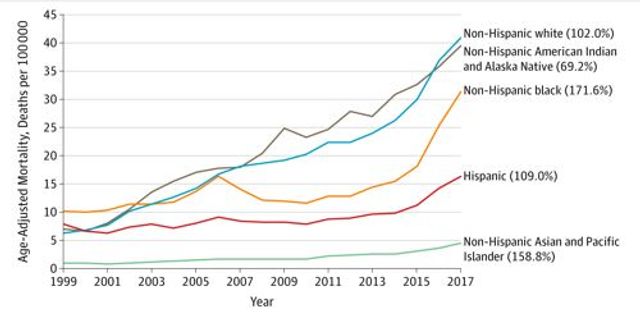
Age-Adjusted Mortality From Unintentional Drug Overdoses, by Race/Ethnicity, US Adults Aged 25-64 Years, 1999-2017. Values in parentheses indicate relative increases in age-adjusted mortality rates by race/ethnicity between 2010 and 2017. Source: CDC WONDER.
Between 1999 and 2017, drug overdose mortality among those in their prime working years increased an astounding 386.5 percent, going from 6.7 deaths to 32.5 deaths per 100,000. The increase in mortality was greatest for the youngest of this cohort, between the ages of 25 and 34, rising 531.4 percent.
The report found that between 2010 and 2017, the overall midlife mortality rate increased from 328.5 to 348.2 per 100,000, resulting in 33,307 deaths that would not have occurred if the rate had held steady.
The rise in mortality has impacted workers across every racial and ethnic group, with the largest number of excess deaths occurring among white workers—a grim refutation of the concept of “white privilege.” By means of such racialist conceptions, the ruling class seeks to promote racial and national divisions even as the reality of social life confirms the fundamental identity of interests of workers of all races and nationalities.
Woolf and Schoomaker found that the largest relative increase in midlife mortality was concentrated in New England and the Ohio Valley, two areas that have been hit particularly hard by deindustrialization and the opioid crisis. Approximately one third of the excess deaths since 2010 occurred in just four states—Ohio, Pennsylvania, Indiana and Kentucky. Eight of the top 10 states for excess deaths are in the Midwest and Appalachia.
“What’s not lost on us is what is going on in those states,” Dr. Woolf told the New York Times. “The history of when this health trend started happens to coincide with when these economic shifts began—the loss of manufacturing jobs and closure of steel mills and auto plants.”
This JAMA analysis exposes the commission of a crime on an immense scale. “When society places hundreds of proletarians in such a position that they inevitably meet a too early and an unnatural death,” Friedrich Engels wrote in 1845 in The Conditionof the Working Class in England, “yet permits these conditions to remain, its deed is murder just as surely as the deed of the single individual.”
The responsibility for driving workers to an early grave lies with the capitalist system’s insatiable demand for ever greater profits. The key accomplices in this crime have been the unions, which serve as the corporations’ industrial police force on the shop floor, ensuring the orderly closure of plants and imposing one concessions contract after another.
In this mad drive for profits, workers are being squeezed past the breaking point. The Amazonifaction of work and the growth of the “gig economy” in the last decade have dramatically increased the exploitation of the working class. Workers are driven to powerful painkillers including oxycontin and opioids simply to cope with the injuries and illnesses that result from overwork.
The reemergence of the class struggle across the US and internationally has shown the way forward. However, while tens of thousands of auto workers, teachers and other workers have taken strike action in the last year, their struggles have been betrayed by the unions.
What is required to meet the needs of the working class is a conscious political leadership with a socialist program on the basis of which workers can take control of the banks and corporations and run them democratically to meet human need, not private profit.
6 Drug Companies’ Role in Opioid Epidemic Scrutinized by Prosecutors
The companies, including Johnson & Johnson and McKesson Corporation, received subpoenas from Brooklyn prosecutors.
Prosecutors asked the companies to hand over documents related to the marketing and sale of opioids. Credit...Spencer Platt/Getty Images
By Nicole Hong
·
·
o
o
o
o
o
Federal prosecutors in Brooklyn have opened a criminal investigation into whether several large drug companies intentionally skirted regulations in order to promote the sale of addictive opioids, according to corporate filings and a person familiar with the matter.
The investigation is part of a heightened law enforcement scrutiny around the country into companies that make and distribute prescription painkillers. Drug companies have faced criminal probes and multibillion-dollar lawsuits for their alleged role in the opioid epidemic.
This year, federal prosecutors in Manhattan and Cincinnati have brought novel cases against companies that distributed opioids to pharmacies, using criminal conspiracy charges typically deployed against drug dealers.
At least six companies disclosed in recent regulatory filings that they received grand jury subpoenas from federal prosecutors in Brooklyn: Johnson & Johnson, Teva Pharmaceutical Industries Ltd., Mallinckrodt PLC, Amneal Pharmaceuticals Inc., AmerisourceBergen Corporation and McKesson Corporation.
Each morning, get the latest on New York businesses, arts, sports, dining, style and more.
Prosecutors from the Eastern District of New York asked the companies to hand over documents related to the marketing and sale of opioids, the filings said. The subpoenas also sought information about the companies’ internal programs and policies to stop the abuse of opioid medications.
Prosecutors are examining whether the companies violated the federal Controlled Substances Act, a broad statute that regulates drug distribution and possession, according to corporate filings and a person familiar with the investigation. The law has been used to impose penalties against pharmacies that failed to adequately control prescription painkillers from reaching the black market.
To bring criminal charges under the statute, the government must prove that the companies or their executives intentionally avoided complying with regulations that require them to flag suspicious orders of opioid medications.
A spokesman for Johnson & Johnson said the company’s procedures for distributing opioid medications complied with the law, adding that monitoring data showed the company’s opioids were rarely abused.
A spokeswoman for Teva said the company was cooperating with the subpoena and was confident in its monitoring policies.
A spokesman for Mallinckrodt declined to comment. Officials at AmerisourceBergen, McKesson and Amneal did not respond to requests for comment.
As deaths from opioid overdoses have surged in the past few years, law enforcement officials across the country have sought to use criminal prosecution against corporate executives accused of contributing to the epidemic. Last year, the Justice Department created a task force to pursue makers and distributors of prescription opioids.
“We will use criminal penalties,” said the United States attorney general at the time, Jeff Sessions. “We will use civil penalties. We will use whatever tools we have to hold people accountable for breaking our laws.”
Opioid cases have become such a priority for the government that the United States attorney for the Eastern District, Richard P. Donoghue, has asked every prosecutor in his criminal division to take on an opioid-related case, according to people familiar with the office.
Earlier this year, for the first time, federal prosecutors in Manhattan brought felony drug-trafficking charges against a major pharmaceutical distributor and two of its former executives. Prosecutors said the former executives at the company, Rochester Drug Cooperative, or RDC, ignored red flags and shipped tens of millions of oxycodone pills and fentanyl products to pharmacies they knew were distributing the drugs illegally.
One of the former executives pleaded guilty to three criminal counts, including intentionally failing to report suspicious bulk orders of fentanyl and other opioids. He is cooperating with prosecutors. The other former executive has pleaded not guilty.
As part of the case, the company agreed to a deal in which it would avoid criminal charges as long as it pays a $20 million fine, complies with the controlled substances law and submits to five years of supervision by an independent monitor.
The company admitted in court papers that it intentionally violated federal narcotics laws by shipping opioids to pharmacies, knowing that the prescription medicines were being sold and used illicitly.
In a similar case in Cincinnati, federal prosecutors this year brought criminal charges against a pharmaceutical distributor, Miami-Luken Inc., saying the company ignored “obvious signs of abuse.” Among other allegations, the government said the company had distributed more than 2.3 million oxycodone pills to a pharmacy in a town of approximately 1,400 people.
The company, which closed, was charged alongside two of its former officials and two pharmacists. All have pleaded not guilty.
Lawsuits around the country have also accused big opioid makers and distributors of using misleading marketing and playing down how addictive the painkillers were in order to increase sales.
 Protesters assemble a makeshift memorial to those lost to drug overdoses last year during a demonstration in support of a proposed supervised injection site, outside the federal courthouse in Philadelphia, in September [Credit: AP Photo/Matt Rourke]
Protesters assemble a makeshift memorial to those lost to drug overdoses last year during a demonstration in support of a proposed supervised injection site, outside the federal courthouse in Philadelphia, in September [Credit: AP Photo/Matt Rourke]
 Age-Adjusted Mortality From Unintentional Drug Overdoses, by Race/Ethnicity, US Adults Aged 25-64 Years, 1999-2017. Values in parentheses indicate relative increases in age-adjusted mortality rates by race/ethnicity between 2010 and 2017. Source: CDC WONDER.
Age-Adjusted Mortality From Unintentional Drug Overdoses, by Race/Ethnicity, US Adults Aged 25-64 Years, 1999-2017. Values in parentheses indicate relative increases in age-adjusted mortality rates by race/ethnicity between 2010 and 2017. Source: CDC WONDER.
No comments:
Post a Comment