GRAPHIC: 74 Killed in
Weeks-Long Cartel War near Texas Border

Tamaulipas
Government
REYNOSA,
Tamaulipas — The raging cartel war for control of this city resulted in at
least 74 officially-counted murders. Many more victims have been incinerated
just south of the Texas border.
In early May, Breitbart Texas
began reporting on rival factions of the Gulf Cartel fighting for control of this border city. The
continuing conflicts resulted in convoys of cartel gunmen roaming the streets looking
for their rivals.
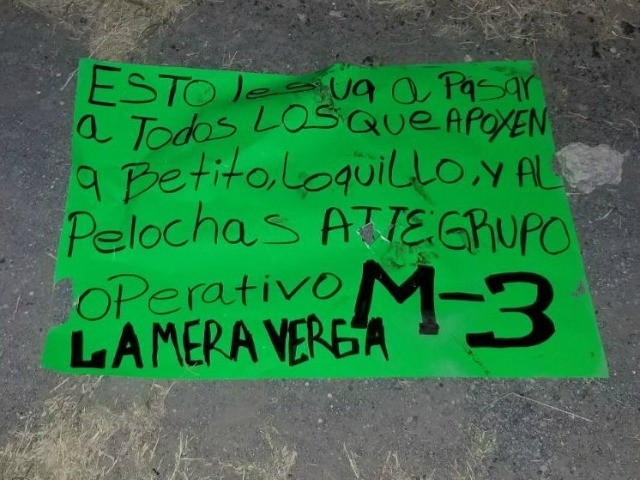
Overnight, cartel gunmen dumped
a bloodied corpse with a posterboard where one cartel factions threatened their
rivals. Bodies with warnings had not been seen previously in
Reynosa. However, they are commonplace in Ciudad Victoria and in the
border state of Nuevo Leon where Breitbart Texas has been reporting Los Zetas
and other cartels are also carrying out massacres.

The violence spiked in early
May, shortly after Mexican authorities killed former Gulf Cartel boss Juan
Manuel “Toro” Loiza Salinas in late April. His death led to a power vacuum
where his former allies are trying to fight off the another faction that
appears to be favored by other cartel leaders. The ongoing fighting has led to a
spike in highway robberies, armed robberies, kidnappings, and extortions as
cartel commanders continue to look for ways to fund their ongoing war.
The raging violence by the Gulf
Cartel immediately south of the Texas border led to the National Border Patrol
Council (NBPC) issuing an alert to agents that they represent regarding the
cartel war just south of the border, Breitbart Texas reported. The NBPC
warned federal agents about the constant gun battles and the possibility of
spillover violence or stray rounds fired in Mexico landing in Texas.
Editor’s Note: Breitbart Texas
traveled to the Mexican States of Tamaulipas, Coahuila, and Nuevo León to
recruit citizen journalists willing to risk their lives and expose the cartels
silencing their communities. The writers would face certain death at the hands
of the various cartels that operate in those areas including the Gulf Cartel
and Los Zetas if a pseudonym were not used. Breitbart
Texas’ Cartel Chronicles are published in both
English and in their original Spanish.
This article was written by “A.C. Del Angel” from Reynosa, Tamaulipas.
MANHUNT: Previously Deported MS-13 Gang Member Allegedly
Murdered Girlfriend

Photo: Harris County Sheriff's Office
HOUSTON, Texas — Law enforcement officials in the Houston area are
searching for a previously deported MS-13 gang member wanted in connection with
the murder of his female companion. The murder victim is also the mother of the
suspect’s child.
The suspect, 26-year-old Carlos
Gonzalez, bragged about killing people and being a member of the hyper-violent MS-13 gang. Just two weeks earlier, the girlfriend’s
sister saw the man “playing” with or “handling” an assault rifle that she said
she thought was an AR-15, according to a criminal complaint obtained by
Breitbart Texas. The preliminary autopsy report indicates she died from
a wound to the head consistent with a rifle round.
Law enforcement officials stated that Gonzalez had been deported
in the past. The victim’s mother said he was from El Salvador. El Salvador is
the home of the MS-13 transnational criminal gang.
Maritza Blanca Lopez sustained a shot to her left front forehead
near the hairline.
“The amount of extensive damage it caused to the skull, and the
trail of fragments and jacketing in the skull was consistent with a rifle
round,” reported the doctor who performed the autopsy at the Harris County
Institute of Forensic Sciences in Houston.
Law enforcement officials discovered Lopez’ partially nude body
after dispatchers received a 911 call from an unknown male “who stated that his
girlfriend was either playing with a gun or checking the gun and accidentally
shot herself.” The man immediately hung up the phone.
Harris County Dispatch called the phone number back, and the
unknown caller said he did not know the exact address but gave them an
intersection in northwest Harris County. He also said he left to take his baby
to the hospital but then decided to take the child to his aunt’s house. He hung
up the phone and did not subsequently answer the phone or call authorities
back.
Patrol deputies went to the scene and found a residence with the
door unlocked. A deputy found an adult Hispanic female in the closet of the
bedroom. She was wearing only panties and a bra. Blood and brain matter was
splattered on hanging clothes, and the walls and the fuse box in the closet. No
weapon, spent-casing, or projectile was found in the closet according to court
documents.
After an investigation, officials determined that Lopez and
Gonzalez were the listed residents on the apartment. A neighbor told officers
that she heard yelling and screaming from two voices in the apartment and then
a “loud boom.”
The murdered woman’s mother, Blanca Garcia said Maritza Lopez
was involved in a domestic disturbance with her daughter the previous night and
has been violent towards Lopez in the past. She said Gonzalez is the father of
her granddaughter and an MS-13 gang member.
Investigators found bloody footprints on the floors and a
balled-up men’s collared shirt on the floor with a lot of blood stains on it.
Lopez first started dating Gonzalez when she was 14-years-old
said her sister, Jessica Lopez. She also told officials that the family had
encouraged her sister to leave Gonzalez.
The dead woman’s sister said her sister told her that the couple
had a fight and she had kicked out Gonzalez and was planning to leave the
apartment. She decided to stay.
Anyone with information about the
5’10” 170 lb. Gonzalez should call Crime
Stoppers Houston at
713-222-TIPS. Officials issued a warrant, but Gonzalez has not been arrested.
There is a $200,000 bond.
Court records obtained from the Harris County District Clerk’s
Officer revealed Gonzalez has a 2010 felony conviction in Harris County for
burglary of a habitation. He also has two pending felony charges for
endangering a child from June 3.
Sheriff’s Office offials and officials with Immigration and
Customs Enforcement confirmed Gonzalez has not been in custody since his
release from prison on the burglary charge.
In March, two MS-13 gang
members appeared in a Harris County courtroom laughing and
waving at news cameras after being charged with the kidnapping and rape of one
14-year-old girl, and the kidnapping, rape, and murder of another young girl in
Jersey Village – a city within the Houston metropolitan area. The murdered girl
was allegedly killed as part of a satanic ritual.
Last Tuesday, William F. Sweeney,
Jr., the assistant director in charge of the FBI in New York told the House
Homeland Security Committee Subcommittee on Counterterrorism and Intelligence,
“MS-13 is not the largest street gang in the United States; it is increasingly
the most violent and well-organized,” reported Breitbart Texas.
The FBI assistant director added that MS-13 members are
“typically much younger than those connected to other street gangs.” They take
“cues from the gang instead of relying on a productive family structure. Also,
those emigrating from El Salvador to the United States are known to be exposed
and desensitized to extreme violence at an early age.” MS-13 members frequently
recruit children who are illegal immigrants.
Breitbart Texas reported that the State of Texas considers the
MS-13 gang to be a Tier 1 level or the “most significant” threat level. The
rise of horrific violence from the gang based in El Salvador and
Honduras has also decidedly affected crime levels in the
fourth-largest city in the United States. Houston is one of the five cities
that the FBI has identified to have a large MS-13 presence. Despite the threat
of MS-13 in Houston and Dallas, Houston Mayor Sylvester Turner and Dallas Mayor Mike Rawlings have
joined other Democrat mayors in Texas in trying to get the law blocked.
Wednesday evening, President
Donald Trump told the crowd
gathered in Iowa that MS-13 was like al-Qaida and stressed again his commitment
to building a border wall, reported The Daily Caller.
In late April Breitbart
News reported that President Trump tweeted, “The
Democrats don’t want money from budget going to border wall despite the fact
that it will stop drugs and very bad MS 13 gang members.”
Bob
Price serves
as associate editor and senior political news contributor for Breitbart Texas.
He is a founding member of the Breitbart Texas team. Follow him on Twitter @BobPriceBBTX and Facebook.
OPEN BORDERS:
HOW THE BANKSTER-FUNDED DEMOCRAT PARTY
NEARLY DESTROYED THE GOP, THE AMERICAN WORKER and then AMERICA!
MEXICANS JUMP AMERICA’S OPEN & UNDEFENDED
BORDERS AMNESTY
"Even though it has gone virtually unreported
by corporate media, Breitbart News has extensively documented the Clintons’
longstanding support for “open borders.” Interestingly, as the Los Angeles Times observed in 2007, the Clinton’s praise for globalization and open borders frequently comes when they are
speaking before a wealthy foreign audiences and donors."
OUR BORDERS ARE NOT OPEN TO NARCOMEX BY ACCIDENT!
SOARING POVERTY AND UNEMPLOYMENT UNDER OBAMA’S OPEN
BORDERS POLICIES.
http://mexicanoccupation.blogspot.com/2016/10/millions-of-americans-legals-unemployed.html
TIME TO CLOSE OUR BORDERS TO NARCOMEX?
"In recent years, the synthetic opioid fentanyl been flooding Dayton and other American cities, trafficked by Mexican cartels who have turned the extremely potent drug into a money-maker."
"In recent years, the synthetic opioid fentanyl been flooding Dayton and other American cities, trafficked by Mexican cartels who have turned the extremely potent drug into a money-maker."
‘Mass-Casualty Event’: Ohio County Now Tops U.S. in Overdose Deaths
THE LA RAZA MEXICAN DRUG CARTELS
BEFORE AND AFTER BARACK OBAMA’S 8 YEARS OF SABOTAGE OF AMERICAN’S HOMELAND SECURITY
MEXICO WILL DOUBLE AMERICA’S POPULATION
THE COUNTY OF LOS ANGELES ALONE HANDS MEXICO’S ANCHOR BABY BREEDERS MORE THAN ONE $$$$ BILLION U.S. DOLLARS PER YEAR…. MORE THAN THE ENTIRE COUNTRY OF MEXICO HANDS THEIR OWN!
How many illegals looting or committing crimes in your county U.S.A.?
IMMIGRANT SHARE OF ADULTS QUADRUPLED IN 232 COUNTIES
"More than 728,000 illegal immigrants have been shielded from being deported and
granted work permits through President Barack Obama’s 2012 executive amnesty
program, according to the Migration Policy Institute."
MEXICO ANNOUNCES CONTROL OF CALIFORNIA ACCOMPLISHED.
De Léon, who introduced the bill, made his remarks at a hearing in Sacramento on SB54, the bill to make California a “Sanctuary State.”
California State Senate President Pro Tem Kevin De Léon (D-Los Angeles) said last Tuesday that “half his family” was in the country illegally, using false documents, and eligible for deportation under President Trump’s new executive order against “sanctuary” jurisdictions.
"The American Southwest seems to be slowly returning to the jurisdiction of Mexico without firing a single shot." --- EXCELSIOR --- national newspaper of Mexico
BELOW LINK IS TO THE LA RAZA “THE RACE” MEXICAN FASCIST SEPARATIST MOVEMENT (WARNING! GRAPHIC!)
They claim all of North America for Mexico!
OPEN BORDERS and HEROIN: AMERICAN POLITICIANS PARTNER WITH THE LA RAZA MEXICAN DRUG CARTELS!
CAUTION!
HERE IS THE MEXICO POURING OVER OUR OPEN AND UNDEFENDED BORDERS AND HAULING BACK BILLIONS FROM HEROIN SALES!
GRAPHIC IMAGES of America coming under Mex Occupation
The NARCOMEX drug cartels now operate in all major American cities and haul back to NARCOMEX between $40 top $60 BILLION from sales of HEROIN!
\
US hospital visits due to opioid issues top one million a year
By Genevieve Leigh
21 June 2017
21 June 2017
A report issued Tuesday by the Agency for Healthcare Research and Quality (AHRQ) shows that there were 1.27 million emergency room visits or inpatient stays for opioid-related issues in 2014, the latest year for which there is sufficient data. This represents a 64 percent increase for inpatient care and a 99 percent hike in emergency room treatment compared to figures from 2005.
Aside from the overall skyrocketing of hospital visits, the report found that the previous discrepancy between males and females in the rate of opioid-related inpatient stays in 2005 has disappeared. The rate of female hospital visits has now caught up to that of males.
Another significant finding is that from 2005 to 2014, the age groups with the highest rate of opioid-related inpatient stays nationally were 25–44 and 45–64 years—in other words, adults in their prime working years, not adolescents. The highest rate of opioid-related Emergency Department (ED) visits was among those aged 25–44 years.
This mirrors another recent report, which found that death rates have risen among the same age group, 25–44, in every racial and ethnic group and almost all states since 2010, likely driven in part by the opioid epidemic.
Using a patient’s area code to estimate the income range of people affected, the researchers were also able to report on differences between the rich and the poor. The results showed that rates of hospital admission or emergency room visits were higher in poorer neighborhoods, but that the increases were uniform, between 75 percent and 85 percent over the 10-year period, across all income ranges.
At the top of the national list for inpatient opioid care is Maryland, which recorded nearly 404 admissions per 100,000 residents. The state, which has been rocked by the epidemic in recent years largely due to the spread of the synthetic opioid fentanyl, has seen a quadrupling of opioid-related deaths since 2010. Baltimore City alone saw 694 deaths from drug and alcohol-related overdoses in 2016—nearly two a day.
Following Maryland, the top 10 states with the highest rate of opioid-related hospital admissions in 2014 were Massachusetts, Rhode Island, New York, West Virginia, Connecticut, Washington, Oregon, Illinois and Maine.
There was substantial state-to-state variation in the findings. States such as Texas, Nebraska and Iowa, for example, are reporting substantially lower rates of hospital admissions than others, which coincides with the unevenness between states in the number of overdose deaths in 2016.
This unevenness may reflect, in part, the ways in which the more potent opioid, fentanyl, has spread throughout the country. The historical divide in the nation’s heroin market between powdered heroin in the East and black tar heroin from Mexico in the West means that fentanyl has been somewhat restricted to certain areas, particularly in the Appalachian and Northeast region.
This does not mean that the opioid epidemic is less severe in the areas with lower hospital visits and deaths rates, only perhaps less deadly. If drug production and distribution makes a shift in the West from black tar to powdered heroin, there will likely be a rise in the use of fentanyl along with it, and consequently the death toll would rise to East Coast levels.
Additionally, the lower rate of hospital visits in rural areas is often due to a lack of access to medical care. Rural areas have even fewer resources to deal with the drug epidemic than their urban neighbors.
Katherine, who works for a nonprofit effort in rural Michigan relating to substance abuse, spoke to WSWS reporters about the unique challenges that face rural areas: “I work in a small rural community with quite a significant opiate crisis just as it is in urban areas. In our county, we don’t have any treatment options. We have one clinic that is limited in what they can do, and it is always at capacity. They [addicts] have to go out of county for treatment, which is about 90 miles away, and there is typically a wait list in these places that are all in major cities. Every place is pretty much running at max capacity all the time.”
If users decide they need help in a rural town it is very likely they will have to wait 72 hours or more before they can get a bed in a rehab, or in a detox facility. Katherine commented on the further challenges that this poses to addicts seeking recovery help: “Around here, if they [a user] are at a point when they are ready—which is a big step and where they often feel very vulnerable—they are basically told to continue using at their regular dosage until something opens up. ... To be told something like that I think makes them lose hope that there is a way out of addiction.”
The obstacles facing workers in the cities are different, but no less severe. Laura, who works in an adult intensive care unit (ICU) in Boston, told the WSWS: “Honestly, one of the hardest things is, even when patients bring themselves in, they have a tendency while detoxing to become verbally or psychologically abusive out of desperation. A detox that ends up in the ICU, which is usually alcoholics because the DTs are life-threatening, is a lot of work. With understaffing in hospitals being what it is, it’s kind of a nightmare.”
Drug users who voluntarily enter the emergency room are almost always looking for a safe place to detox, an extraordinarily painful and traumatic process. Patients going through withdrawal from opioids experience vomiting, uncontrollable shaking, sweating, cramping, diarrhea, insomnia, anxiety, intense cravings, etc.
Most hospitals do not have options for patients who wish to detox. Some doctors are actually authorized to prescribe patients an additional drug called suboxone to help with the symptoms. However, without support and supervision this treatment option often proves to be a futile and even dangerous one. Reports of suboxone abuse, and even overdoses, have spiked significantly since the onset of the crisis.
Laura explained the limitations that exist even for hospitals that provide resources for detox: “We have a detox unit. But it can’t do much for patients who are acutely withdrawing. If they score over a certain number on the scales that we use, they get transferred to the regular hospital units. And we don’t have addiction training. … Addicts are a underserved and vulnerable population.”
Health care workers in both rural and urban areas express frustration over the seemingly endless crisis. The sheer breadth of the opioid epidemic is astounding. It has bled into nearly every major social challenge of the day, putting a strain not only on hospital and emergency workers, but also on social welfare programs, the education system, mental health facilities, child care workers and more. This creates a situation where the drug epidemic, itself the product of a diseased social order, becomes a major contributor to its further decay.
The capitalist system as a whole is the source of the drug abuse epidemic, as any combination of the various strands of social ills affecting an individual could lead to substance abuse and addiction. The scope of the crisis represents a very complex manifestation of the problems created by a society in which every aspect of life is subjugated to private profit and where only an infinitesimal fraction of the resources available are directed to meet social need.
Katherine in Michigan touched on this reality in her comments to the WSWS: “I think that there are so many people who are suffering, experiencing poverty and extreme hardship, or who are encountering prejudice and oppression, and these factors are all compounding to create the basis for the drug epidemic to flourish. It is such a multifaceted issue. People are feeling extremely helpless watching the events in society and the political situation, and it is almost like a building up of unrest underneath the surface.”

